Posterior Cervical Foraminotomy
Introduction
Cervical spine disease is a fairly common problem seen in adults. When that disease involves the compression of spinal nerves in the neck, people may seek advice from their doctor. Symptoms can range from mild neck pain to severe numbness in the hand and electric-like pain shooting down the shoulder, arm, and hand. Some patients can even experience significant weakness in the arm or hand. Fortunately, most people can be treated successfully without surgery or aggressive treatment. In a few patients, however, these symptoms can persist despite conservative treatment or become so severe that surgery is recommended for relief. Anterior cervical discectomy and fusion (ACDF) is a well known procedure to address such a problem. It involves going through the front of the neck and removing disc material from a spinal level and then stabilizing that level by placing bone graft material and metallic hardware. When the spine is fused, there is no longer motion at that level. Posterior cervical foraminotomy is an alternative surgical procedure to relieve symptoms of a pinched spinal nerve. This procedure is performed through the back of the neck and it creates more space for the spinal nerve to pass through. In properly selected patients, posterior cervical foraminotomy is as effective as ACDF surgery without requiring a fusion procedure.
Anatomy
The spine is composed of three basic elements: bones, named vertebrae; intervertebral discs, which act as shock absorbers between the vertebrae; and nerve tissue, the spinal cord and nerve roots. The vertebrae are hollow bones which look like rings. They are stacked one on top of another to form a column with a central canal. The discs separate one vertebra from another and they serve to cushion the spinal column. The spinal cord is fairly delicate, and it is protected as it runs from the brain down through the canal of the bony vertebral column. The nerve roots are nerve branches that exit from both sides of the spinal cord, and they travel out of the spinal column through boney passages called foramen. The spinal cord resembles a tree trunk while the individual nerve roots look like branches of the tree. Once out of the spine, the nerve roots travel to various parts of the body to relay information. In the neck, there are seven vertebrae, and eight pair of cervical nerve roots.
Cervical Spine Disease
In cases of cervical spine disease, discs can weaken and bulge or even rupture to cause pinching or compression of either the spinal cord or more commonly, particular nerve roots. The bone itself can wear out and then develop spurs which also compress the spinal cord or nerve roots as they pass through their foramen. Spinal cord compression is a serious problem and it usually requires surgical intervention. Nerve root compression if significant can also be problematic, and it may also require treatment by a spinal surgeon. You may experience neck pain; neck stiffness; numbness in the hands; weakness in the arms or hands; or pins and needles sensation in the arms and hands, called radiculopathy. The severity of these complaints can vary and in some cases can worsen with time. You may be referred to a spinal surgeon as the symptoms progress. A spinal surgeon can assess the extent of the cervical disease process by listening to your description of the symptoms, by conducting a thorough physical examination, and by studying the results of radiographic studies, such as MRIs or CT/myelograms. The decision to operate is made with great care and with your permission if non-operative care is unsuccessful.
Procedure
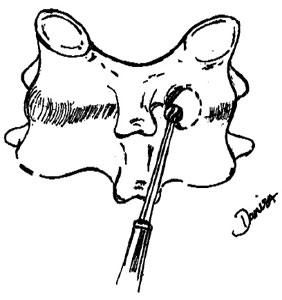
Posterior cervical foraminotomy relieves spinal nerve root compression by creating more room for the nerve root to pass through the foramen. When disc material compresses the nerve root on one side (unilateral compression), the cervical foraminotomy can be used to remove the portion of the offending disk. When a bone spur narrows the foramen and compresses the nerve root, a posterior cervical foraminotomy can be used to chisel away the spur to widen the passageway. Some refer to this procedure as minimally invasive, in that the incision is relatively small and no fusion of the spine is required.