Explore
If you are diagnosed with a spinal disorder, deformity, or potential problem that can by helped through the use of external structural support, your physician may recommend the use of a neck or back brace. Neck and back braces are most often used to treat low back pain, trauma, infections, muscular weakness, neck conditions, and osteoporosis. They immobilize and support the spine when there is a condition that needs to be treated. Depending on the model that is used, they can put the spine in a neutral, upright, hyper-extended, flexed, or lateral-flexed position.
Spinal braces are used for a variety of reasons - to control pain, lessen the chance of further injury, allow healing to take place, compensate for muscle weakness, and prevent or correct a deformity. They offer a safe, non-invasive way to prevent future problems or to help you heal from a current condition. Though the effects of bracing are primarily positive, they can lead to a loss of muscle function due to inactivity. Bracing can sometimes lead to psychological addiction, so that even when a person is healed and ready to be taken off the back brace, he or she feels dependent upon it for physical support.
The use of braces is widely accepted. They are effective tools in the treatment of spine disorders. In fact, more than 99% of orthopedic physicians advocate using them.
Braces are not new - they have actually been around for centuries. Lumbosacral (lum-bo-sack-ral) corsets (for the lower back) were used as far back as 2000 B.C.! Bandage and splint braces were used in 500 A.D. to treat scoliosis. Recently, braces have become a popular way to help prevent primary and secondary lower back pain from ever occurring.
There are more than 30 types of back supports available for spine disorders. Some of the most common types are described below:
Neck Braces
Neck braces stabilize the cervical spine after neck surgery, trauma to the neck, or as an alternative to surgery. They are the type of spinal brace you most commonly see people wearing. There are several types available, including:
- Soft Collar - a flexible brace placed around the neck. It is typically used after a more rigid collar has been worn for the major healing. It is used as a transition to wearing no collar.
- Philadelphia Collar - a more rigid/stiff collar with front and back pieces that attach with Velcro on the sides. It is usually worn 24 hours a day until your physician instructs you to remove it. This collar is used for conditions such as a relatively stable cervical fracture, cervical fusion surgery, or a cervical strain. Another similar type is the Miami cervical brace.
- Sterno-Occipital (stern-oh-ox-ip-ital) Mandibular(man-dib-you-lar) Immobilization Device (SOMI) - a brace that holds your neck in a straight line that matches up with your spine. It offers rigid support to a damaged neck and prevents the head from moving around. With this brace, you are unable to bend or twist your neck. The restriction of motion helps the muscles and bones to heal from injury or surgery.
- Halo - a brace used to immobilize the head and neck. This is the most rigid of the cervical braces. It is only used after complex cervical spine surgery or if there is an unstable cervical fracture. The halo looks a lot like the word sounds. It has a metal ring (halo) that goes around your head and secures to your skull with four metal pins. The ring then attaches by four bars to a vest that is worn on your chest to bear the weight of the brace. The Halo is worn 24 hours a day until the spine injury heals.
Back Braces
- Trochanteric (trow-can-ter-ick) Belt - usually prescribed for sacroiliac joint pain or to stabilize pelvic fractures. The belt fits around the pelvis, between the trochanter (a bony portion below the neck of your thigh bone) and the iliac (pelvis) ridges or crests. The belt is about five to eight centimeters wide and buckles in front, just like a regular belt.
- Lumbosacral (lum-bo-sack-ral) and Sacroiliac (sack-ro-ili-ack) Belt - helps to stabilize the lower back. It is usually made of heavy cotton reinforced by lightweight stays. The pressure can be adjusted through laces on the side or back of the belt. Lumbosacral belts range in widths from 10 to 15 centimeters, and 20 to 30 centimeters. The sacroiliac belt is used to prevent motion by compressing the joints between the hipbone and sacrum at the base of the spine.
- Corset - provides rigid support for the back. Corsets vary in length. A short corset is typically used for low back pain, while a longer one is used for problems in the mid to lower thoracic spine. When people think of corsets, they usually conjure up images of women from earlier centuries who used them to make their waists look smaller. Today, in the treatment of back problems, corsets refer to a type of back brace that extends over the buttocks and is often held up by shoulder straps. Like the corsets of old, these corsets lace from the back, side, or front. There are metal stays that provide the appropriate rigidity and support for the back.
- Rigid Brace - usually prescribed for low back pain and spinal instability when standard back supports are not stiff enough. Rigid braces usually have upright pieces in the rear that curve to the shape of your lower spine and pelvis, with bands across the thoracic region of your spine. There are also fabric straps on the braces that provide pressure in the front. Some common types of rigid braces are:
- Williams Brace - a rigid brace with no vertical uprights in the middle, allowing you to bend.
- Chair-back Brace - a rigid brace that holds the lumbar spine in the neutral position and limits sideways and rotating movement of the lower spine.
- Raney Flexion Jacket - a rigid brace that reduces curvature of the lumbar spine by holding it in a neutral tilt.
- Hyperextension Brace - designed to prevent excessive bending. Hyperextension braces are often prescribed to treat frontal compression fractures that have occurred where the thoracic and lumbar areas of the spine meet. They can also be used after surgery for spinal fusion, taking pressure off the anterior or front of the thoracic vertebrae by restricting flexion (bending) of the thoracic and lumbar spine. Hyperextension braces have a front rectangular metal frame that puts pressure over the upper sternum or breast bone and the pubic bone, allowing the spine to extend. The brace also applies pressure over the T-10 level (the tenth vertebra in your thoracic spine). The hyperextension brace braces provides what is called "three-point stabilization" to the spine through a front abdominal pad, a chest pad, and a rear pad at the level of the fracture. The most common types of hyperextension braces are Knight Taylor and Jewett.
- Molded Jacket - designed to distribute pressure widely over a large area. It stabilizes the spine from the neck to the hips, distributing pressure evenly and taking excess pressure off overloaded or unstable areas. The molded jacket was originally made of plaster of Paris. Now it is usually made of molded plastic.
- Lifting Belt - designed to reduce low back strain and muscle fatigue that can occur when you are lifting heavy objects. It circles around your waist, covering the lumbar region of your spine, and closes in the front. Lifting belts are usually made of cloth or canvas and do not have stays. Some models also have lordosis pads to contour to the curvature of your spine.
Another method for relieving pressure on the spinal cord that may be causing spinal stenosis or cervical myelopathy is to remove the front of the spinal canal. This means that the large part of several of the vertebrae must be removed - the vertebral bodies and the discs between. This procedure is called a corpectomy. "Corpus" means body and "ectomy" means remove. Once the vertebral bodies have been removed, the space must be filled with something. Just as in the anterior cervical fusion, this space is usually filled with a bone graft. Some type of internal fixation is usually required to hold the vertebrae and the bone graft in place. You will probably also need to be placed in a halo jacket to hold your head perfectly still while the healing occurs and the vertebrae fuse.
"Discectomy" means "remove the disc". A discectomy relieves the pressure on a nerve root by removing the herniated disc causing the pressure.
The discectomy procedure is performed through an incision down the center of the back over the area of the herniated disc. The muscles are moved to the side so that the surgeon can see the back of the vertebrae. X-rays may be required during surgery to make sure the correct vertebra is located. The surgeon cuts a small opening through the lamina (lam-in-ah) bone on the back of the spinal column. This procedure, called "laminotomy," is used to give the doctor room to see and work inside the spinal canal.
The nerve roots are moved out of the way. Upon locating the problem disc, the surgeon removes it, easing pressure and irritation on the nerves of the spine. Small instruments that fit inside the disc are used to remove as much of the nucleus as possible. This prevents the remaining disc material from herniating in the future.
After the discectomy, the muscles of the back are returned to their normal position around the spine. The skin incision is repaired with sutures or metal staples. In some cases, a discectomy may be combined with a spinal fusion, where the two vertebrae above and below the removed disc are joined together or fused.
Exercise is vital to recovery and to maintaining a healthy spine. Consider it part of long-term health management and risk reduction. Regular exercise is the most basic way to combat back and neck problems. However, if you already have an injury or damage to your spine, talk to your doctor or physical therapist (PT) before you start an exercise routine, to make sure the exercises you choose are effective and safe for your particular case.
Why exercise? Scientific studies show that people who exercise regularly have far fewer problems with their spine. Exercise helps strengthen the muscles in your back that connect to your spine. Exercise can reduce your risk of falls and injuries. It can also strengthen your abdomen (your belly), arms, and legs, which reduces back strain. Stretching reduces risk of muscle spasms. In addition, weight bearing exercises help prevent loss of bone mass caused by osteoporosis, reducing your risk of fractures. Aerobic exercise, the type that gets your heart pumping and pulse rate up, has been shown to be a good pain reliever as well. The natural chemicals of the body that combat pain - called endorphins (en-dor-fins) - are released during exercise and actually reduce your pain.
Exercises will help maximize your physical abilities including:
- Flexibility - exercises that increase flexibility help to reduce pain and make it easier to keep your spine in a healthy position. Flexibility exercises are helpful for establishing safe movement. Tight muscles cause imbalance in spinal movements, which can make it easier to injure your spine. Gentle stretching increases flexibility, eases pain, and reduces the chance of re-injury.
- Stabilization - "core" muscles are the muscles located closer to the center of your body and act as stabilizers. These key muscles are trained to help you position your spine safely and to hold your spine steady as you perform routine activities. These muscles form a stable platform, which allows you to move your arms and legs with precision. If the stabilizers are not doing their job, your spine may be overstressed by daily activities.
- Coordination - strong muscles need to be coordinated. As the strength of the spinal muscles increases, it becomes important to train these muscles to work together. Learning any physical activity takes practice. Muscles must be trained so that the physical activity is under control. Spine muscles that are trained to control safe movement help reduce the chance of re-injury.
- Conditioning - improving your overall fitness level will help you recover from spine problems. Fitness conditioning involves safe forms of aerobic exercise. The term aerobic means "with oxygen." When using oxygen as they work, muscles are better able to move continuously, rather than in spurts. Examples of aerobic exercise include:
- Swimming laps
- Walking on a treadmill
- Using a cross country ski machine
- Using a stair stepper
If you decide you want some extra conditioning, always check with your doctor or therapist before beginning a program on your own. It is important that you choose an aerobic activity you enjoy. This will help you stick with it, so you reap the long-term benefits that come with a well-rounded exercise program.
If spinal stenosis is the main cause of your neck pain, then the spinal canal must be made larger and any bone spurs pressing on the nerves must be removed. One way that this is done is with a complete laminectomy (lam-in-eck-toe-mee). Laminectomy means "remove the lamina". The lamina is the back side of the spinal canal and forms the roof over the spinal cord. Removing the lamina gives more room for the nerves and lets the surgeon remove any bone spurs from around the nerves. A laminectomy reduces the pressure on the spinal cord and relieves the irritation and inflammation of the spinal nerves.
In the cervical spine, removing the lamina completely may cause problems with the stability of the facet joints between each vertebra. If the joints are damaged during the laminectomy, the spine may begin to tilt forward, causing problems later. One way that spine surgeons try to prevent this problem is to not actually remove the lamina. Instead, they simply cut one side of the lamina and fold it back slightly. The other side of the lamina opens like a hinge. This makes the spinal canal larger giving the spinal cord more room. The cut area of the lamina eventually heals to keep the spine from tilting forward.
Aspirin
Aspirin is available without a prescription, and can help relieve minor pain and back ache. The main potential side effect of aspirin is stomach problems, particularly ulcers with or without bleeding. You should not take aspirin if you are pregnant; in fact, you should not take any medication unless you have discussed the medication with your obstetrician.
NSAIDs (Non-Steroidal Anti-Inflammatory Drugs)
NSAIDs are available without a prescription and include ibuprofen, acetaminophen, and naproxen. They are very effective in relieving the pain associated with muscle strain and inflammation. They block the inflammatory response in joints. However, NSAIDs can affect your kidneys, especially if you are elderly. Excessive use on NSAIDS can lead to kidney and liver problems. Do not take NSAIDS if you are pregnant.
Non-Narcotic Prescription Pain Medication
Non-narcotic pain medication, or "analgesics" (the term analgesics means "pain relievers") treat pain at the point of injury. They are used for treating mild to moderate chronic pain. Non-narcotic analgesics that require a prescription from the doctor include NSAIDs such as, carprofen, fenoprofen, ketoprofen, and sulindac. To reduce the chance of side effects when taking non-narcotic prescription medications, do not lie down for 15 to 30 minutes after taking the medication, and when you are outside, avoid direct sunlight, and wear protective clothing and sun block. Avoid using these medications if you are pregnant, or have recurrent ulcers or liver problems.
Narcotic Pain Medications
If you have severe pain, your doctor may prescribe a narcotic pain medication such as codeine or morphine. Narcotics relieve pain by numbing the central nervous system. The strength and length of pain relief differs for each drug. Narcotics can cause side effects such as nausea, vomiting, constipation, and sedation or drowsiness. These side effects are predictable and may be prevented by taking the following steps:
- Do not take sleeping aids or antidepressants when you are taking a narcotic pain medication
- Avoid drinking alcohol
- Increase your fluid intake
- Eat a high-fiber diet
- Use a fiber laxative or stool softener to treat constipation
Remember - narcotics can be addictive if used excessively or improperly.
Muscle Relaxants
Muscle relaxants can help relieve pain from muscle spasms. However, they are not completely effective, and can cause drowsiness and depression. Muscle relaxants should typically only be taken for three or four days. Long-term use is not recommended.
Antidepressants
Back pain is a common symptom of depression. Antidepressants can relieve emotional stress that leads to symptoms of back pain. An important fact to note - the same chemical reactions in the nerve cells that trigger depression also control the pain pathways in the brain. Some antidepressant medications are believed to reduce pain by affecting this chemical reaction in the nerve cells. Some types of antidepressants also make good sleeping medications. If you are having trouble sleeping due to your back pain, your doctor may prescribe an antidepressant to help you get back to a normal sleep routine. Antidepressants can have several side effects such as, drowsiness, loss of appetite, constipation, dry mouth, and fatigue.
Epidural Steroid Injections (ESI) - Nerve Block
An ESI can be used to relieve the pain of stenosis and irritated nerve roots, as well as to decrease inflammation. Injections can also help reduce swelling from a bulging or herniated disc. The steroid injections are a combination of cortisone (a powerful anti-inflammatory medication) and a local anesthetic that are given through the back into the space between the facet joint. Epidural steroid injections are not always successful in relieving symptoms of inflammation. They are used only when other conservative treatments have failed.
Minimally invasive spine surgery is an approach in which special surgical instruments are used to see inside the body and perform surgery without the need for a large incision. The increase in minimally invasive spine surgery techniques has been made possible by advances in lasers, endoscopy (en-dos-co-pee), and image guidance systems.1 Although there are risks associated with any type of surgery, including minimally invasive spine surgery, minimally invasive spine surgery offers several advantages over traditional open surgery approaches. The advantages of minimally invasive spine surgery include:
- Less muscle injury 2
- Less blood loss 2
- Less post-operative pain
- Faster rehabilitation 2
- Smaller scar
- Shorter hospital stay 2
- Faster return to activities of daily living including work 2
Not all types of spine surgery can be performed using a minimally invasive technique, and minimally invasive spine surgery is not recommended for everyone. If your doctor has recommended spine surgery, ask whether minimally invasive spine surgery may be right for you.
1 Jaikumar S, Kim DH, Kam AC. History of minimally invasive spine surgery. Neurosurg. 2002;51(5 Suppl):S1-S14.
2 Datamonitor. Stakeholder opinions: Minimally invasive spinal surgery. Product Code: DMHC1938. Published Dec-03. Available at: http://www.datamonitor.com. Accessed: July 5, 2006.
The goal of spinal fusion surgery is to stabilize your spine, reduce back pain and lessen leg pain. Minimally invasive techniques offer exciting new options for patients. The decision to have surgery requires careful thought. Your surgeon can advise you and answer your concerns. Read this brochure to answer your basic questions. Write down any questions you may have and decide with your surgeon if minimally invasive lateral spinal fusion is right for you.
Why is a spinal fusion performed?
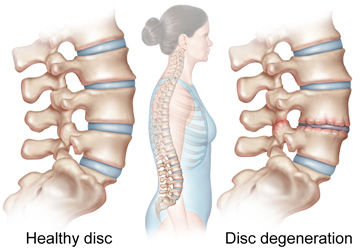
Your spine is subject to constant wear and tear. Soft rubber-like discs between the bones in your spine cushion and protect your spine as you perform daily activities. Back pain can occur when one or more of these discs wear out or become damaged by injury or disease, such as degenerative disc disease or DDD. Spinal fusion is performed to stabilize the spine and reduce or remove the pain by removing the disc and joining two or more vertebral bones together.
What makes a minimally invasive lateral fusion different?
The minimally invasive lateral procedure for spinal fusion is performed through a small incision in your side rather than your back. This protects the muscles in the back from being cut during the surgery. Minimally invasive surgery may have many potential advantages when compared to traditional open spine surgery:
- Smaller incisions and smaller scars
- Less surgical blood loss
- Shorter hospital stay
- Less pain and pain medicine during recovery
What happens during surgery?
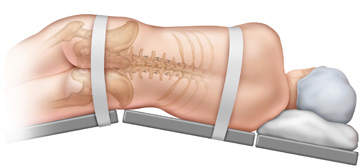
You will be placed on the operating table on your side and you will be taped to the table so that your body doesn't move during the surgery.
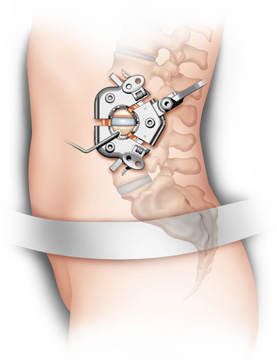
Your surgeon will place a special instrument called a retractor into the incision in your side and surgically tunnel down to your spine.
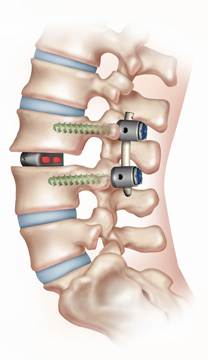
With other special instruments your surgeon will remove the disc that is causing your pain. In place of the disc, your surgeon will insert an implant holding bone graft. After the fusion procedure, your surgeon may also place other devices such as small screws and rods through small incisions in your back. The implants will help stabilize the spine while the bones are fusing together and your body heals.
What happens after surgery?
Your pain will be treated by medication and you will likely remain in the hospital for 1-3 days. During your recovery you will see your surgeon for follow-up appointments and start a physical therapy program. Talk to your surgeon about when you can start to resume daily activities and return to work. Upon healing, you will have one small scar on your side and small scars on your back from your incisions.
What are the benefits and risks?
Each patient is unique so no two will respond to surgery in the same way. Potential benefits include a decrease or elimination of your pain and a return to your normal activities. As with any major surgery there is a risk of complications such as continued pain, infection, nerve damage, or the need for surgery in the future. Talk to your surgeon to make sure you understand the benefits and risks of any surgical procedure.
With any surgery, there is a risk of complications. When surgery is done near the spine and spinal cord these complications (if they occur) can be very serious. Complications could involve additional pain and impairment and the need for additional surgery. You should discuss the complications associated with surgery with your doctor before surgery. The list of complications provided here is not intended to be complete and is not a substitute for discussing the risks of surgery with your doctor. Only your doctor can evaluate your condition and inform you of the risks of any medical treatment he or she may recommend.
- Anesthesia - any surgery that requires anesthesia can be potentially harmful. Surgery on the cervical spine usually requires that you be put under general anesthesia. General anesthesia means that you are put to sleep. Anesthesia carries a risk of allergies to the medications. There are also different life-threatening situations that can occur during anesthesia. It is extremely unlikely that these complications will occur, but you should be aware that they are possible.
- Infection - any surgery involving an incision in the skin can become infected. In addition, the bone graft and area around the spine may become infected. An infection will usually require some type of antibiotic medication to treat the infection. If the infection involves the bone, it may require one or more additional surgeries to drain the infection. The risk of infection is usually less than one percent.
- Blood Vessel Damage - there are large arteries and veins that travel through the neck into the brain. The carotid artery and the jugular vein are nearby. It is possible to damage these blood vessels during the surgery. Again, it is extremely unlikely that this will occur, probably less than one in a thousand.
- Nerve Damage - there are nerves in the neck that travel along the area where the incision is made to perform an anterior cervical discectomy and fusion. These nerves go to the vocal chords. There is the possibility that these nerves can be damaged during surgery. This can lead to hoarseness. If this occurs, it will usually recover unless the nerve is permanently damaged or cut. Again, this is unlikely.
- Spinal Cord Damage - surgeries that are performed on the cervical spine place the spinal cord at risk for injury. Spinal cord damage is probably much more likely in the larger, more serious operations such as the corpectomy and strut grafting procedures. These are complex, difficult operations and are done for extremely serious problems that are unlikely to respond to any other type of treatment. Routine anterior discectomy and fusion are common surgeries that are extremely safe. While damage to the spinal cord is possible, it is highly unlikely.
- Graft Displacement - one of the more common problems that can occur after an anterior cervical discectomy and fusion is that the bone graft may move out of position. If it moves too much, it may require a second surgery to place a new bone graft in its place.
- Non-Union - in spite of a successful surgery and good bone graft, a fusion may not occur between the vertebrae. This is termed a non-union or pseudarthritis. Usually your surgeon will be able to tell whether a fusion has occurred by looking at X-rays taken over a three- to six-month period after surgery. If a fusion does not occur and you have no pain, a second surgery will not be necessary. If you continue to have pain, and a non-union is diagnosed after surgery, your surgeon may suggest a second attempt at fusion. When trying for the second time after a failed fusion, most surgeons will usually include some type of internal fixation, such as a plate and screws.
The type of spine surgery you have will determine how long you will need to stay in the hospital and how much help you will need in and out of the hospital after surgery. Many procedures for the spine only require one to three nights in the hospital.
What Can I Expect While in the Hospital?
From the moment your spine surgery is completed, the nursing staff will begin monitoring your condition. When the anesthesia begins to wear off, you will be taken to a hospital room until you are ready to go home.
Day 1
The day after surgery is considered "Day 1." Some spine surgeries require that you wear a brace for a period of time afterward. If so, keep your brace on until your surgeon specifically instructs you to remove it. You may be encouraged to stand and sit (with assistance if needed) within the first 24 hours after surgery. If so, with the supervision of a physical therapist (PT), you will sit on the edge of the bed and stand with support. Walking, however, will be approached gradually and carefully to avoid injury and complications. Try not to over do it the first few times you get up and walk.
- Treatments - a nurse will check the circulation and motion of your legs and feet. You may be given a spirometer (sper-ah-ma-ter) (a tube you breathe into) to help expand your lungs and prevent pneumonia. Surgical tape, sutures, or adhesive tape will have been used to close your incision. This dressing may be removed and changed. An ice pack or cooling pad may be used to help decrease swelling and increase your comfort. It is common to continue intravenous (IV) fluids for the first day or two.
- Medications - you may be given antibiotics through your IV for the first 24 hours to help prevent infection. Pain medication will be made available to help relieve any pain or discomfort you may be having. During the first 24 hours after surgery, you will probably be given pain medications that are injected into your IV line or directly into your arm or buttock. These medications are usually much stronger and faster acting than pills taken by mouth. Tell your nurse if you are uncomfortable due to pain. It is important to keep your pain in check so you can participate in your rehabilitation program.
- Diet - how quickly you recover from anesthesia varies from person to person. Your diet will be ordered by your doctor at first, and it will be adjusted as your intestinal function gets back to normal. Usually you will be allowed to have clear liquids as soon as you are able to eat. If you feel okay after drinking clear liquids, you will be given food that is more solid. Special precautions will be taken if you had surgery from the front of your neck.
- Activities - your PT will work with you to begin moving safely in bed and up to a sitting position. You will gradually progress to standing and walking. You may require the use of a walking aid (cane or walker) for a short time. He or she may suggest exercises to relieve soreness in your legs, such as tightening and releasing your thigh and buttock muscles and pumping your ankles back and forth to keep fluid from pooling in the lower limbs and help prevent blood clots.
- Tests - you may need to have blood checked every day if your doctor has placed you on blood thinning medications. These tests are needed to regulate anti-coagulant (blood thinning) therapy. During the first few days, your doctor will monitor your blood thinning level.
Day 2
By your second day in the hospital after spine surgery, you may expect the following:
- Treatments - your IV line may be removed. If you have a urinary catheter, that may also be removed. You will probably continue to use the spirometer to help prevent pneumonia, and your wound dressing may be changed or removed.
- Medications - it is natural to feel some pain during the first few days after spine surgery. The pain can usually be controlled with medication, so let your nurse know if you are in pain. By Day 2, you will begin switching from medications given through injection or your IV to pills that can be taken by mouth. Taking medications by mouth will make things easier when you are ready to go home.
- Activities - it is important to continue doing the exercises that have been prescribed by your doctor or PT to help improve motion and keep your muscles from getting sore and tight. Ice packs may be applied before and after therapy treatments to reduce swelling and relieve pain. With assistance from your PT, you will gradually increase the distance you are walking in preparation for going home.
Day 3 and Beyond
- Treatments - your wound dressing will be changed if needed or removed.
- Activities - your physical therapy will continue to focus on safety with mobility, with the goal of enabling you to be independent. In spite of any mild discomfort, it is important that you do your deep breathing and exercises as instructed. Breathing and moving well will help improve your lung capacity and circulation, and may help you heal faster. You will be able to return home when your doctor feels that your medical condition is stable. You may be instructed to limit your activities for a period of time to give your body a chance to heal. As you prepare to leave the hospital, be sure to follow the instructions given by your health care team.
What Can I Expect When I Get Home?
After spine surgery, people often report feeling better soon after they awake from the surgery. Although you may see and feel immediate benefits, you will get the maximum benefits of surgery by participating in a comprehensive rehabilitation program. When you are leaving the hospital, your doctor or PT may recommend some or all of the following to help you get better at home:
- Ice and Heat - cold treatments are usually recommended in the first few days after surgery. Ice makes blood vessels vasoconstrict (vase-oh-con-strict) (get smaller), decreasing the blood flow. This helps control inflammation, muscle spasm, and pain. Heat may also be recommended. Heat makes blood vessels vasodilate (vase-oh-dye-late) (get larger), increasing the blood flow. This helps flush away chemicals that cause pain. It also helps bring in healing nutrients and oxygen.
- Relaxation - pain after spine surgery can be physically and emotionally draining. Relaxation exercises can help you control pain and the stress that comes with it. You may be given instructions for breathing exercises to help air reach even deep into your lungs. You may also be instructed to slow your breathing to a more relaxed pace. Slower breathing can help muscles relax, while bringing much needed oxygen to sore tissues.
- Rest - giving your body a chance to rest can help ease soreness after surgery, giving your spine time to heal. Follow your doctor's instructions for using any prescribed supports or braces.
- Positioning - your PT may suggest ways to position your spine for greater comfort. These positions may include the use of pillows or towels to support your spine and help take pressure of the surgical area.
- Movement - careful movements suggested by your PT can safely ease pain by providing nutrition and lubrication in the areas close to the surgical area. Movement of joints and muscles also signals the nervous system to block incoming pain. Using safe body movements can help you avoid extra strain on your spine in the weeks after your spine surgery.
- Lying in Bed - avoid lying in positions that twist or angle your spine. Do not curl up in the "fetal" position. Choose a firm mattress. Do not lay on a soft bed or sofa. Keep enough pillows nearby to support your head, shoulders, trunk, and legs.
- Moving in Bed - when getting in or out of bed, use the "log roll" technique. To get out of bed, roll onto your side and sit up while keeping your spine steady and secure. Instead of twisting your upper body when you roll to one side, try to roll your whole body as a unit, like rolling a log. Then let your legs ease off the edge of the bed toward the floor as you push yourself up into a sitting position. This reduces strain from twisting your spine and gives the surgical area time to heal. To get into bed, do just the opposite: sit first with your legs hanging off the side of bed, then lie on your side and roll like a log onto your back.
- Sitting - keep your spine upright and supported when sitting. A safe, upright posture reduces strain on your spine. Choose a chair that supports your spine. Avoid soft couches or chairs. Place a cushion or pillow behind your back while driving or riding in a car. When standing up, keep your spine aligned by leaning forward at the hips.
- Bending - your doctor or PT may tell you not to bend for a few weeks after spine surgery. Always follow your doctor's instructions. If and when you are given the okay to bend, do so safely. Keep your back straight and secure as you bend forward, making sure your spine is straight. Consider using a "grabber" to avoid bending over at the waist to put on socks or shoes, and to pick up items from the floor.
- Lifting - your doctor may tell you not to lift or carry anything for a period of time after surgery. Do not test your back by trying to lift or carry anything until your doctor says it is okay. If you must pick up or carry lighter items, squat down by bending your knees. Do not lean forward by bending your spine forward. Keep the item close to your body, even if it is light. Holding the weight out in front of you puts extra strain on your spine. Check with your doctor or PT if you have any questions about the safety of lifting or carrying.
- Outpatient Therapy - your doctor may prescribe outpatient rehabilitation once your condition has begun to stabilize. Your recovery from spine surgery can be improved by learning new ways to strengthen your spine and prevent future problems. Your PT will teach you ways to help reduce your pain now, and help you develop new habits to keep your spine healthy.
If physical therapy is recommended, your physical therapist (PT) will start by asking you questions about your spine condition. You may be asked questions about when your pain started, where you hurt, and how your symptoms affect your daily activities. Your answers will help your PT focus on the source of your problem and what he or she will need to do to help relieve it. You PT will then likely do an exam that may include some or all of the following checks.
- Posture - imbalances in the position of your spine can put pressure on sore joints, nerves, and muscles. Improving your posture can often make a big difference in relieving pain.
- Range of motion (ROM) - measurements are taken of how far you can move in different directions. Your ROM is recorded to compare how much improvement you are making with each treatment.
- Nerve Tests - your PT may check your reflexes, sensation, and strength. The results can help determine which area of the spine is causing problems and the types of treatment that will be best for you.
- Manual Exam - your PT will carefully move your spine in different positions to make sure that the joints are moving smoothly at each level. Muscle and soft tissue flexibility is also tested.
- Ergonomics - ergonomics involves where and how you do your work or hobby activities. By understanding your ergonomics, your PT can learn whether the way you do your activities may be making your pain worse. Sometimes even simple corrections can make a big difference in easing spine problems.
- Palpation - your PT will feel the soft tissues around your spine to check for changes in temperature or texture, which may indicate that you have inflammation or nerve irritation. Palpation also checks whether there are tender points or spasms in the muscles near the spine.
Your PT will evaluate your answers and your exam results to decide the best way to help you. He or she will then write a plan of care, which lists the treatments to be used and the goals that you and your PT decide on to do your daily activities safely and with the least amount of discomfort. The plan also includes a prognosis, which is your PT's idea of how well the treatments will work and how long you will need therapy in order to get the most benefit.
To control pain and symptoms, your PT may recommend the following physical therapies:
- Rest - resting painful joints and muscles helps calm soreness, giving your spine time to heal. If you are having pain with an activity or movement, it should be a signal that there is still irritation going on. You should try to avoid all movements and activities that increase the pain. In the early stages of your therapy, your doctor or PT may have you wear a brace to limit movement.
- Specific Rest - specific rest allows safe movement of the joints and muscles on either side of a painful area while protecting the sore spot. If a brace was prescribed, you may be instructed to take it off a few times each day so you can do some gentle and controlled exercises.
- Positioning - your PT will help you find positions for your spine that are most comfortable while sleeping or resting. He or she may also suggest positions to reduce stress on your spine while you are at work.
- Ice - ice makes blood vessels constrict or get smaller, which decreases the blood flow. This helps control inflammation, muscle spasm, and pain.
- Heat - heat makes blood vessels dilate or get larger, which increases the blood flow. This helps flush away chemicals that cause pain, and also helps bring in healing nutrients and oxygen.
- Ultrasound - ultrasound uses high-frequency sound waves to reach sore muscles and other tissues that are over two inches below the surface of your skin. As the sound waves pass through your body they vibrate molecules, causing friction and warmth. This heating effect helps flush the sore area and brings in a new supply of blood that is rich in nutrients and oxygen.
- Electrical Stimulation - electrical stimulation gently stimulates nerves as the current passes through pads applied on the skin. Some people say it feels like a massage on their skin. Electrical stimulation can ease pain by sending impulses to your brain that are felt instead of pain. Once the pain eases, muscles begin to relax, letting you move and exercise with less discomfort.
- Soft Tissue Massage - PTs are trained in many different forms of soft tissue massage. Massage has been shown to reduce pain and spasm by helping muscles relax, by bringing in a fresh supply of oxygen and nutrient-rich blood, and by flushing the area of chemical irritants that come from inflammation. Soft tissue massage can help tight muscles relax, getting them back to a normal length. This will help you begin to move with less pain and greater ease.
- Joint Mobilization - your PT may apply changing pressures and movements to your joints to help lubricate joint surfaces. This will ease stiffness and help you begin moving with less pain. As your pain decreases, more vigorous pressures and movements may be used to lengthen tissues around the joint in order to restore better movement in your spine.
- Traction - sore joints and muscles often feel better when traction (pull) is used. PTs apply traction with their hands or with a traction machine. There are also traction devices that you can use at home. The amount of pull that is needed will depend on your condition. A gentle on/off pressure may be better early on to help control arthritis pain. More vigorous traction can help take away pain if a spinal joint is mildly sore or tight.
PTs use functional training when you need help doing specific activities with greater ease and safety. Examples of functional training include:
- Posture - healthy posture keeps your spine in safe alignment, reducing strain on the joints and soft tissues around your spine. The time and effort you take to use good posture are vital to spine care, and will help to prevent future spine problems. As you regain strength and control, proper posture and body alignment will be easier to remember and apply with all your activities.
- Body Mechanics - think of body mechanics as putting safe posture into action. It is one thing to sit or stand with good posture, but another to keep safe posture as you actually move with activity. You want to keep your body in its safest alignment as you go about your daily tasks, such as getting out of a chair, taking out the trash, getting clothes out of the dryer, brushing your teeth, and lifting. Safe body movement is especially important during lifting. To avoid extra spine strain when lifting, use these safety tips:
- Plan and prepare for the lift
- Make sure you have good footing
- Straddle your feet with a wide base of support
- Keep the load close to your body
- Keep your spine stable and aligned
- Do not twist or pivot with your feet
- Ergonomics - Ergonomics looks at the way people do an activity. It is possible that even minor changes in the way you do your work or hobby activities could keep your pain and symptoms in check, while protecting your spine from further injury. Ergonomics doesn't usually involve expensive changes. Even minor adjustments in the way you do your activities can make a huge difference in easing your pain and preventing further problems.
Once your pain is controlled, your range of motion has improved, and your strength is returning, you will be able to continue your physical therapy on your own at home. Your PT will review some of the ideas listed above to help take care of any soreness at home. You will be given instructions to help you keep working on your range of motion and strength. Before you are done with therapy, more measurements may be taken to see how well you are doing now compared to when you first started therapy.
Spinal fusion is usually performed after a discectomy, The goal of spinal fusion is to stop the motion caused by segmental instability. This reduces the mechanical pain caused from excess motion in the spinal segment.
In this procedure, the surgeon fills the space left after the disc is removed with a block of bone called a bone graft. This graft may be taken from your pelvis, or it may be obtained from a bone bank. Bone graft from a bone bank is given by organ donors and stored under sterile conditions until it is needed for operations such as spinal fusion. The bone goes through a rigorous testing procedure, similar to a blood transfusion. This is in order to reduce the risk of passing on diseases, such as AIDS or hepatitis, to the recipient.
Illustration of a spinal fusion (cross-section).
Placing a bone graft between two or more vertebrae causes the vertebrae to grow together, or fuse. If your back or neck pain is caused by segmental instability, a spinal fusion may also be recommended even if you do not have radiculopathy.
When doing a spinal fusion, the bone graft may simply be wedged in tight between the vertebrae, which holds the graft in place. In recent years, there has been an increase in the use of metal plates, pedicle (ped-i-cul) screws, and rods to try to improve the success of the fusion. Many different types of metal implants are used, and all of them try to hold the vertebrae in position while the fusion heals. Bone heals best when it is held still, without motion between the pieces trying to heal together. The healing of a fusion is no different than healing a fractured bone, such as a broken arm. In particular, the cervical spine is a difficult part of the body to hold still.
There are two basic types of spinal fusion:
Anterior Interbody Fusion
In the anterior (which refers to the front side of your body) interbody fusion, a bone graft is placed between two vertebrae after the disc is removed. During the healing process, the vertebrae grow together, creating a solid piece of bone out of the two vertebrae. When surgery is needed, the anterior interbody cervical fusion is used to treat most problems in the neck caused by degenerative disc disease. These include unrelieved neck pain and pressure on the nerve roots caused by bone spurs or a herniated disc.
Bone Graft to Provide Support
Bone graft is also used for structure. Rather than crush the bone into fine pieces, larger pieces of bone are used to fill a gap between two bones. For example, if the surgeon removes a vertebra or disc, he or she may place a chunk of bone graft into the space. Because bone is rigid, it will hold the bones apart while the body grows to the ends of the graft. Over time the entire piece of bone that was grafted will be "remodeled" and replaced by the body with new bone. The time it takes to fuse depends on the size of the piece of bone that was used. It is sometimes a slow process that may take several years.
Types of Bone Used in Bone Graft
Two types of bone are used in bone graft procedures: autograft (auto-graft), which is bone taken from your own body; and allograft (al-oh-graft), which is bone that comes from a bone bank. The most common approach is to use your own bone whenever possible. Sometimes your surgeon may mix allograft with autograft.
Allograft can come from many types of bones and in many different forms. Allograft is usually removed from organ donors and placed in bone banks. Bone banks test it for diseases such as hepatitis and AIDS - just like testing done in a blood bank. Allograft does not contain any living cells, so it has fewer chemicals to stimulate growth of new bone. The disadvantage of an allograft is that it may not always grow as well or as quickly as an autograft, but a bone-growing protein can be added to the area to make up for what the bone graft lacks. The advantage to using allograft is that you do not have to donate the bone graft. This makes your surgery shorter, and there may be less pain afterward. The allograft carries a very small risk of transferring infectious diseases even though it is carefully tested.
Allograft is very useful when your operation requires more bone graft than your own body can supply. Some major spine fusions need a lot of bone graft. Some surgeries need large pieces of structural bone graft, which may cause problems in the area of your body where the bone was removed.
Advancements in Bone Graft Technology
Much research is being done to design bone graft substitutes, chemicals, and devices that stimulate the bones to fuse. It is well known that electrical current stimulates bone to grow. Many surgeons use electrical stimulation devices during the first weeks after surgery to speed up fusion. Some artificial bone graft materials have been developed. For instance, sea coral, harvested from oceans, is sometimes used as a structural bone replacement. Other developments include:
- Demineralized bone matrix (DBM) - a type of allograft developed from bones in a bone bank. The bone has the calcium removed and can be turned into a putty, sheet, or gel. The material can then be added to a graft site to improve the fusion.
- Autologous growth factor (AGF) - a solution used to stimulate bone growth. It is created in a laboratory from blood platelets (the clotting part of blood). The mixture is usually used in combination with some form of structural support, such as autograft or fusion cages.
- Bone morphogenic protein (BMP) - a chemical added to bone graft to improve bone growth when it is added to a fusion site.
Total disc replacement (TDR) may be a solution for some people with degenerative disc disease as an alternative to spinal fusion. Early research into artificial disc replacement began in the 1960s. Interest was renewed in the 1990s because of the complications sometimes caused by spinal fusion. Since then, research and design efforts on total disc replacement have increased significantly.
During disc replacement surgery, the surgeon removes the damaged disc and replaces it with an artificial disc. The goals of total disc replacement surgery are to:
- Maintain segmental spinal motion
- Relieve pain and increase activity
- Restore disc height and proper spine curvature
- Reduce post-operative recuperation time
- Reduce risk of bone graft donor site pain and pseudarthrosis (sewd- arth-row-sis), which is improper movement of a joint after healing
Posture at work, rest, and play affects the health of your back and neck. Posture is a result of proper body mechanics - which occurs when your spine goes from the healthy neutral position into action.
STEP 1: Understand the Neutral Back Position
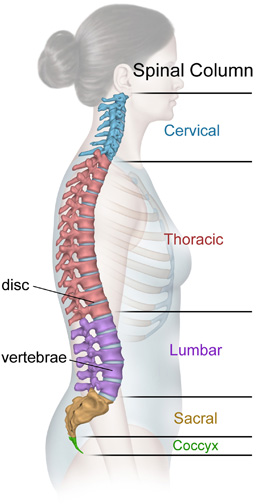
A healthy spine as three natural curves:
- The neck, or cervical spine, curves slightly inward
- The mid back, or thoracic spine, is curved outward
- The low back, or lumbar spine, curves inward
These natural curves are the result of the muscles, ligaments, and tendons that attach to the vertebrae of the spine working together in harmony. Without these supporting structures, the spine would collapse. They support the spine just as guide wires support the mast of a ship.
In your spine, the guide wire system is made up mainly of the abdominal and back muscles. The abdominal muscles provide support by attaching to the ribs, pelvis, and indirectly to the lumbar spine. The muscles of the back are arranged in layers, with each layer playing an important role in balancing the spine. By using these muscles together, you can change the curves of your spine, like when you bend over to pick something up.
Neutral alignment keeps the muscles, ligaments, and tendons that attach to your spine working together in harmony. This is important to help cushion your spine from too much stress and strain. Learning how to maintain a neutral spine position can help you avoid problems with your spine, and help you move safely during activities like sitting, walking, and lifting.
Controlling the tilt of your pelvis is one way to help balance your spine. As certain muscles of the back and abdomen contract, the pelvis rotates. As the pelvis rotates forward, the lumbar curve increases. As the pelvis rotates backward, the curve of the low back straightens. Rotation of the pelvis is like a wheel centered at the hip joint. The muscles of the upper thighs also attach to the pelvis and contraction of these muscles can be used to change the curve of the spine.
The abdominal muscles work alone or with the hamstring muscles to rotate your pelvis backward. This causes the slight inward curve of the low back to straighten. If these muscles cause the curve of the low back to straighten too much, this may produce an unhealthy slouching posture.
In the other direction, the hip flexor and back extensor muscles rotate the pelvis forward. This increases the curve of your lower back. If this curve is increased too much, another unhealthy posture may result.
A balance of strength and flexibility is the key to maintaining the neutral spine position. This balance ensures the best muscle function. Like a car, an imbalance may lead to wear and tear, eventually damaging the various parts of the car.
Muscle imbalances that affect the spine have many causes. One common cause of muscle imbalance is weak abdominal muscles. As the abdominal muscles sag, the hip flexors become tight, causing an increase in the curve of the low back. Another common problem results from tight hamstrings. As the hamstring muscles become tight, the pelvis is rotated backwards. This produces an abnormal slouching posture.
STEP 2: Put Safe Posture Into Practice
Sitting
Healthy sitting posture is based on the neutral spine position. Positioning your hips and knees at 90 degrees can help you keep a neutral sitting posture. This position is balanced between the extremes of lumbar movement. Remember to choose a properly designed chair to help support your lumbar spine. The neutral spine position is also important when getting up from a chair. Holding your spine safely in neutral, the pelvic wheel turns forward, placing the "nose over the toes". With the feet placed shoulder width apart, stand upright. Use the buttock and thigh muscles to push yourself up. Do not twist or bend too far over at the waist, or you will put too much strain on your lumbar spine.
Walking
Proper body mechanics are also important while walking. Try to maintain the neutral spine position while walking. In the neutral position, your legs and arms swing naturally during forward motion. Conditions that alter the normal way of walking, and cause a limp, can severely stress the spine. While walking, always try to maintain your spine in the neutral position.
Lifting
Lifting is one of the most dangerous activities for your spine. The neutral spine position MUST be used to reduce the risk of injury. With your spine in the neutral position, movement occurs as the pelvic wheel turns. The hip is the axis of pelvic rotation, not the back! Notice how the back loses the neutral position when the pelvis does not rotate forward. This posture focuses the force on your back muscles during a lift. Lifting in a neutral position allows the larger and more powerful leg muscles to do the lifting. When lifting, first find the neutral position. Bend at the hips by rotating the pelvic wheel at the hip joint axis. Keep the safe posture, hold the object securely, and use your large leg muscles to generate power. Tighten your abdominal muscles during the lift to create a stabilizing corset around your trunk.
- Pay Attention to your Body: If something you are doing causes your back to hurt, stop and rest or stop altogether. Whether it is a particular exercise, prolonged sitting, bending, or twisting, listen to your body's signals. Pain is a warning. Discuss the activity with your doctor or physical therapist before proceeding.
- Sit and Sleep Comfortably: Be sure that your back and neck are properly supported when you sit or sleep. When you sit, make sure your lower back is supported. Talk to your health care provider about choosing an appropriate mattress and pillow. You can upset the alignment of your spine if a mattress is too soft, or a pillow too high.
- Lose Weight: If your weight is causing excessive pressure to your spine, weight loss can reduce your discomfort.
- Lift Properly: Do not lift heavy loads by placing the pressure on your lower back. Use your legs to lift, and always bend your knees so your arms are at the same level as the heavy object you plan to lift. This simple technique will save your back unnecessary wear and tear.
- Avoid Osteoporosis: Talk with your physician about combating the affects of osteoporosis - bone thinning. Possible treatments include weight bearing exercise, adequate calcium and vitamin D, and hormone replacement therapies.
Many back injuries occur during lifting. To help protect your back and avoid painful injury, follow these safer lifting tips:
- First, plan and prepare for the lift. It only takes a moment to ensure your safety, but the pain of a back injury can be long lasting!
- Ensure you have a safe and clear path.
- Before beginning, think through the lift.
- Get a good footing with a wide base of support by placing your feet a minimum of shoulder width apart. This lowers your center of gravity and increases your stability.
- Keep the load close! Keeping the load you are lifting close to your body can reduce stress on your spine and back muscles. Think of how a lever and fulcrum works. Your back muscles, spine, and arms are the parts that form this lever system. The force needed to lift an object is lower if the load is nearer the fulcrum point. If the load is too far away from your body, the muscles of your spine have to work harder to help with the lift. This puts too much stress on the muscles of your spine and can cause injury.
- Maintain the neutral spine position! By moving the pelvic wheel around its axis, your upper body hinges forward while your spine stays in neutral. Keep the neutral spine position at all times!
- Remember to lift with the large muscles of your legs!
- Do not twist and bend your lower back at the same time! This is one the most damaging movements to the spine. To avoid twisting, pivot your feet to complete the lift.
- Get help if necessary! If the load is too bulky or heavy, do not hesitate to get help or use a hand truck! Do not be too tough or too busy to get help. Will power does not take the place of a reasonably safe lift.
Whether you are at work or at home, it is common to feel stress and tension. Today, people are often called on to do more with fewer resources. They are faced with more responsibility and more deadlines to get their tasks done. The health of your neck may be at risk with these mounting pressures. But scientists have helped us learn that we have a defense against these mounting pressures - the "Three R's" for easing tension and reducing neck pain at home and work:
- Rest - taking frequent breaks during the work hour, and choose alternate activities to get your mind ready for a new job task such as deep breathing, walking, napping, or exercising.
- Relaxation - take a load off. Lie back. Turn down the lights, and listen to your favorite tape or CD. Breath slowly and deeply, allowing your abdomen to rise and fall rhythmically. Using visual imagery can also aid in relaxation. Try to visualize each muscle relaxing one after another.
- Recovery - repeated and prolonged activities can take their toll if your body does not get a chance to recover. Recovery helps repair sore, aching tissues along the way, keeping them healthy.
Here are some additional tips you can use to avoid tension at work and keep your back and neck healthy:
- Be Relaxed - try to keep your muscles relaxed. To stay relaxed, look relaxed.
- Pace Yourself - keep an even keel. Avoid sudden changes in your workload. Try to avoid last minute "panics" to meet deadlines.
- Take a Break - take a thirty second "microbreak" every twenty to thirty minutes to do some deep breathing and a few exercises. Take a few minutes each hour to do some exercises, get a drink, or go bug a coworker. Use your lunch break to take a nap or a walk.
- Change Positions - avoid holding your neck, trunk, or limbs still for a long time. Plan ways to get the job done using different positions. Sit for a bit, then stand for a bit. Or simply readjust your approach to the task.
- Rotate Duties - rotating or sharing your tasks can be fun by offering a new work setting while giving your body a chance to recover.
- Avoid Caffeine and Tobacco - caffeine (in coffee, tea, soda, and chocolate), and tobacco can increase stress, reduce blood flow, and increase your awareness of back and neck pain.
Vertebroplasty (ver-tee-bro-plas-tee) and kyphoplasty (kye-fo-plas-tee) are surgical treatments your doctor may recommend that are specificly for spinal compression fracture.
- Vertebroplasty - a minimally invasive procedure in which special cement is injected into the broken vertebral body. This treatment is mainly used to ease pain and improve the strength of the vertebral body.
- Kyphoplasty - a minimally invasive procedure in which a tube with a deflated balloon is slipped inside the broken bone. Once inside, the balloon is inflated to help restore the height of the broken vertebra. Then bone cement is injected into the space formed by the balloon to hold the vertebra at its corrected height.